Source: The Conversation – USA (2) – By Gonzalo Maturana, Associate Professor of Finance, Emory University

The U.S. government shutdown couldn’t come at a worse time for federal workers.
With a government shutdown, hundreds of thousands of federal employees would be furloughed – sent home without pay until funding resumes. And ahead of the shutdown, President Donald Trump suggested that a prolonged lapse in funding could open the door to “irreversible” changes, such as reducing parts of the federal workforce.
The shutdown marks another difficult moment this year for a federal workforce that has so far shed more than 300,000 jobs. This is largely due to ongoing Trump administration efforts to downsize parts of the federal government and restructure or largely eliminate certain government agencies with the stated aim of increasing efficiency.
As a team of financial economists who study labor markets and public sector employment and have examined millions of federal personnel records spanning such government shutdowns in the past, we have found that the consequences reach far beyond the now-familiar images of closed national parks and stalled federal services. Indeed, based on our study of an October 2013 shutdown during which about 800,000 federal employees were furloughed for 16 days, shutdowns leave an enduring negative effect on the federal workforce, reshaping its composition and weakening its performance for years to come.
What happens to workers
Millions of Americans interact with the federal government every day in ways both big and small. More than one-third of U.S. national spending is routed through government programs, including Medicare and Social Security. Federal workers manage national parks, draft environmental regulations and help keep air travel safe.
Whatever one’s political leanings, if the goal is a government that handles these responsibilities effectively, then attracting and retaining a talented workforce is essential.
Yet the ability of the federal government to do so may be increasingly difficult, in part because prolonged shutdowns can have hidden effects.
When Congress fails to pass appropriations, federal agencies must furlough employees whose jobs are not deemed “excepted” – sometimes commonly referred to as essential. Those excepted employees keep working, while others are barred from working or even volunteering until funding resumes. Furlough status reflects funding sources and mission categories, not an individual’s performance, so it confers no signal about an employee’s future prospects and primarily acts as a shock to morale.
Importantly, furloughs do not create long-term wealth losses; back pay has always been granted and, since 2019, is legally guaranteed. Employees therefore recover their pay even though they may face real financial strain in the short run.
A cynical observer might call furloughs a paid vacation, yet the data tells a different story.
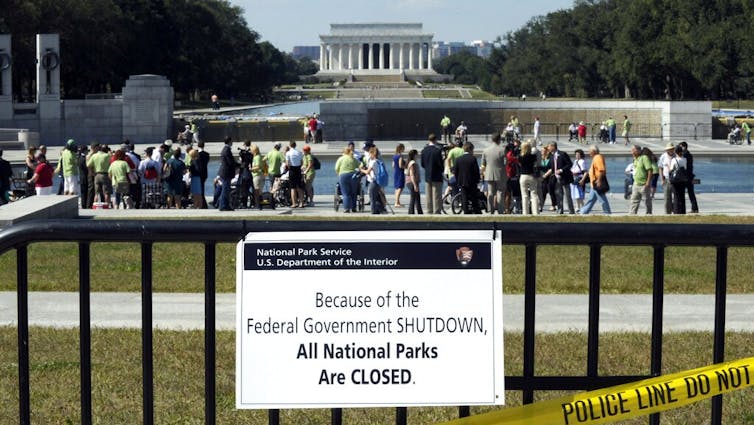
AP Photo/Susan Walsh
Immediate consequences, longer-term effects
Using extensive administrative records on federal civilian workers from the October 2013 shutdown, we tracked how this shock to morale rippled through government operations. Employees exposed to furloughs were 31% more likely to leave their jobs within one year.
These departures were not quickly replaced, forcing agencies to rely on costly temporary workers and leading to measurable declines in core functions such as payment accuracy, legal enforcement and patenting activity.
Further, we found that this exodus builds over the first two years after the shutdown and then settles into a permanently lower headcount, implying a durable loss of human capital. The shock to morale is more pronounced among young, female and highly educated professionals with plenty of outside options. Indeed, our analysis of survey data from a later 2018-2019 shutdown confirms that morale, not income loss, drives the exits.
Employees who felt most affected reported a sharp drop in agency, control and recognition, and they were far more likely to plan a departure.
The effect of the motivation loss is striking. Using a simple economic model where workers can be expected to value both cash and purpose, we estimate that the drop in intrinsic motivation after a shutdown would require a roughly 10% wage raise to offset.
Policy implications
Some people have argued that this outflow of employees amounts to a necessary trimming, a way to shrink government by a so-called starving of the beast.
But the evidence paints a different picture. Agencies hit hardest by furloughs turned to temporary staffing firms to fill the gaps. Over the two years after the shutdown we analyzed, these agencies spent about US$1 billion more on contractors than they saved in payroll.
The costs go beyond replacement spending, as government performance also suffers. Agencies that were more affected by the shutdown recorded higher rates of inaccurate federal payments for several years. Even after partial recovery, losses amounted to hundreds of millions of dollars that taxpayers never recouped.
Other skill-intensive functions declined as well. Legal enforcement fell in agencies that became short of experienced attorneys, and patenting activity dropped in science and engineering agencies after key inventors left.
Official estimates of shutdown costs typically focus on near-term GDP effects and back pay. But our findings show that an even bigger bill comes later in the form of higher employee turnover, higher labor costs to fill gaps, and measurable losses in productivity.
Shutdowns are blunt, recurring shocks that demoralize the public workforce and erode performance. These costs spill over to everyone who relies on government services. If the public wants efficient, accountable public institutions, then we should all care about avoiding shutdowns.
After an already turbulent year, it is unclear whether a shutdown would significantly add to the strain on federal employees or have a more limited effect, since many who were considering leaving have already left through buyouts or forced terminations this year. What is clear is that hundreds of thousands of federal employees will experience another period of uncertainty.
This story was updated on Oct. 1, 2025, to include details of the shutdown.
![]()
The authors do not work for, consult, own shares in or receive funding from any company or organization that would benefit from this article, and have disclosed no relevant affiliations beyond their academic appointment.
– ref. Even a government shutdown that ends quickly would hamper morale, raise costs and reduce long-term efficiency in the federal workforce – https://theconversation.com/even-a-government-shutdown-that-ends-quickly-would-hamper-morale-raise-costs-and-reduce-long-term-efficiency-in-the-federal-workforce-265723































{kind=link}
{kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
.jpg){kind=link}
{kind=link}