Source: The Conversation – USA – By Justin Dunnavant, Assistant Professor of Anthropology, University of California, Los Angeles
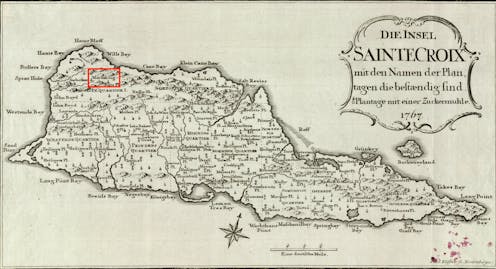
“For a long time now, a large number of [escaped slaves] have established themselves on lofty Maroon Hill in the mountains toward the west end of the island [of St. Croix]. … They are there protected by the impenetrable bush and by their own wariness.”
Those are the words of Christian Oldendorp, a Danish missionary who visited the Caribbean island of St. Croix in 1767. His account is one of the few Danish historical records of Maronberg, a community of escaped slaves, known as Maroons, in the northwest mountain ranges of the island.
In 1733, the Danish West India-Guinea Company purchased St. Croix from France and quickly expanded the island’s sugar and cotton production. This also meant expanding the slave population to harvest lucrative plantations. But the Danes were never able to fully control the island – or the enslaved. By the end of the 1700s, nearly 1,400 people – more than 10% of the enslaved population – successfully escaped captivity. But where did they escape to? Only recently have researchers started to shed more light on this centuries-old mystery.
As an archaeologist specializing in slavery and resistance, I’ve excavated plantations in the Americas and used geographic information systems to model Maroon escape routes by sea. Recently, I turned my attention to Maroon settlements on land, working with a team of archaeologists to locate Maronberg.

Justin Dunnavant, CC BY
Honoring a legacy
I first learned about Maronberg on a nature tour of St. Croix given by local activist and University of the Virgin Islands professor Olasee Davis in 2016. At that time, I was on the island to excavate a sugar plantation, a project that gave my colleagues and me a unique perspective on the enslaved experience in the Danish-controlled Caribbean.
In August 2025, Davis’ decades-long campaign to create an official heritage sanctuary to protect Maronberg finally came to fruition. The local government purchased 2,386 acres of land to serve as the U.S. Virgin Islands Maroon Territorial Park.
But one problem remains: We have yet to find the physical remains of the settlement. Locating and preserving Maronberg’s historical artifacts and buildings could provide new insight into residents’ way of life and give greater meaning to the sanctuary.
Fortunately, advanced computer modeling and high-resolution maps are helping us get closer to pinpointing the settlement.
Finding what was meant to remain hidden
Many Maroon settlements in the Americas have proved difficult to locate. This makes sense when you consider that their inhabitants were trying to hide from colonial settlers. If the Danes had found Maronberg, they would have either killed its inhabitants or forced them back into slavery.
Runaways tended to settle in areas that were intentionally difficult to access, like remote swampy or mountainous terrain. Houses and other shelters often consisted of semipermanent structures so that Maroons could relocate as needed to avoid detection.
The boundaries of Maronberg and the size of the settlement along the northwestern mountain range remain unknown. Colonial militias attempted periodic raids, but historical records report that they were met with rugged terrain, booby traps and counterattacks.
The missionary Oldendorp wrote: “[The Maroons] keep every approach safe by attempting carefully to conceal small, pointed stakes of poisoned wood so that the unwary pursuer might wound his foot on them and therefore be prevented from continuing the chase as a result of the unbearable pain.”
All those precautions paid off: The Danes were never able to penetrate the Maroons’ encampment.
Using new tech to see 300 years into the past
Recent attempts by researchers to locate Maronberg began in 2007, with more extensive geographic information systems mapping conducted in 2008. These digital, computer-based geographic programs allow researchers to store a range of geological data and model spatial patterns across vast terrains.
Pairing a historical map with a low-resolution elevation map from the U.S. Geological Survey, archaeologist Bo Ejstrud created a predictive model to assess the probable location of the Maroon settlement. He considered elevation, slope and colonial infrastructure to identify the most remote areas of St. Croix with the least visibility from colonial lines of sight.
Back in the 1700s, urban centers accounted for only a small percentage of the overall landmass of the 83-square-mile (215-square-kilometer) island. Much of the land was either plantations or uninhabited forests and mountains. Ejstrud’s model reaffirmed the likelihood of a Maroon settlement in the northwest region. But it left us with a massive survey area. The map also didn’t account for the possibility that the settlement moved over time.
In 2020, I teamed up with archaeologists Steven Wernke, from Vanderbilt University’s Spatial Analysis Research Laboratory, and Lauren Kohut, from Winthrop University’s Geospatial Environmental Modeling Lab. Together, we developed and visualized a more dynamic model using advances in mapping since 2008.
We began by digitizing two of the most detailed colonial maps of St. Croix – one from 1750 and another from 1799. These maps, created by Danish military engineers and surveyors, detail the spread of plantations, roads and settlements over time.
Next, in order to build a digital elevation model of the island’s terrain, we incorporated high-resolution light detection and ranging, or lidar, data collected by the National Oceanic and Atmospheric Administration. Whereas traditional digital elevation models can be skewed by dense vegetation and trees, lidar uses laser pulses that penetrate through the forest canopy to map the Earth’s surface. This technology allows us to analyze some of the most secluded, inaccessible areas on the island. Prior to 2013, lidar was too costly for archaeological research purposes. But these days, it’s built into many cellphones.
By layering these datasets in geographic information systems software, we created a suitability model that estimated where Maroon settlements were most likely to have existed. In addition to isolation and visibility, we also incorporated accessibility to water sources and terrain ruggedness to model the degree of mobility through the landscape.
This approach allowed us to simulate how the opportunities and constraints the landscape offered to people seeking refuge shifted as colonial society grew over time.

Lauren Kohut, Steven A. Wernke and Justin Dunnavant, CC BY
Mapping changes
In addition to providing more nuance to the picture of the areas where Maroons potentially settled, our research suggests that the Maroon settlement wasn’t static, but likely waned as colonial infrastructure increased on the island. Our model implies that the area of suitable land for clandestine Maroon communities shrank by more than 90% in just 50 years.
It’s possible that over time there were fewer runaways. More likely, more Maroons left the island by boat for destinations such as Puerto Rico and Tortola.
Where we go from here
Though our findings still don’t provide an exact location for Maronberg, they get us one step closer to locating the physical remains of this centuries-old Maroon community. The next step will be to visit these sites and survey them for evidence of historical settlement. Archaeological research at these sites would help us understand more about the Maroons who turned a rugged landscape into a sanctuary for freedom.
Ultimately, identifying artifacts and historical sites within the newly established U.S. Virgin Islands Maroon Territorial Park would help us develop educational tours and honor the Maroon legacy.
![]()
Justin Dunnavant does not work for, consult, own shares in or receive funding from any company or organization that would benefit from this article, and has disclosed no relevant affiliations beyond their academic appointment.
– ref. Escaped slaves on St. Croix hid their settlements so well, they still haven’t been found – archaeologists using new mapping technology are on the hunt – https://theconversation.com/escaped-slaves-on-st-croix-hid-their-settlements-so-well-they-still-havent-been-found-archaeologists-using-new-mapping-technology-are-on-the-hunt-237291



















{kind=link}